
We’re all gonna die of something, right?
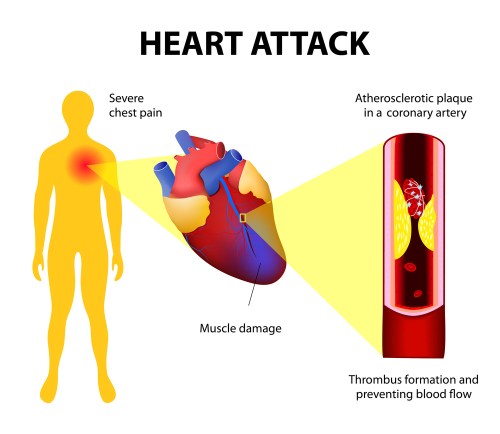
The #1 cause of death in the U.S. is coronary artery disease (CAD), which causes heart attacks and sudden cardiac death. Blockage in the heart arteries typically develops over years and many people are walking around not knowing it’s there. The lucky ones develop warning signs like chest pain or shortness of breath on exertion. After consulting a physician, the next step may be a “stress test” or some sort imaging of the arteries of the heart.
Angiography refers to imaging of arteries or veins. Angiography of the heart arteries is helpful in diagnosing blockage of arteries that may cause heart attacks or sudden cardiac death in the future.
CT stands for computerized tomography: x-rays obtain images that are then manipulated by computer technology to provide more information than plain x-ray technology alone. CT angiography of the heart arteries is done with iodinated contrast injected into the low-pressure venous system of circulation. In contrast, standard arterial angiography involves introduction of a needle (and catheter) into the high-pressure arterial system, usually the femoral artery in the groin or the smaller radial artery in the wrist. Standard arterial angiography is associated with a higher risk of complications such as leakage of blood from the artery. Another potential complication is embolization of arterial plaque or clots downstream from the arterial puncture. Because of the higher complication rate in the arterial system, standard angiography is considered “invasive.”
The study at hand asks which is a better way to image heart arteries in a patient with stable chest pain: CT versus standard arterial angiography. The article abstract doesn’t define “stable” chest pain. I assume the researchers did not include acute myocardial infarctions (heart attacks) and unstable angina.
European researchers concluded that:
Among patients referred for invasive coronary angiography (ICA) because of stable chest pain and intermediate pretest probability of coronary artery disease, the risk of major adverse cardiovascular events was similar in the CT group and the ICA group. The frequency of major procedure-related complications was lower with an initial CT strategy.
I bet the non-invasive CT is also less expensive that standard arterial angiography.
Steve Parker, M.D.


Click to purchase at Amazon.com. E-book also available at Smashwords. com.


