Posted onJanuary 27, 2022|Comments Off on Anti-Aging: Glycine and N-acetylcysteine
The following article tempts me to take supplemental glycine and N-acetylcysteine. I also wonder if they would help counteract the cyktokine storm of serious COVID-19.
Cellular increases in oxidative stress (OxS) and decline in mitochondrial function are identified as key defects in aging, but underlying mechanisms are poorly understood and interventions are lacking. Defects linked to OxS and impaired mitochondrial fuel oxidation, such as inflammation, insulin resistance, endothelial dysfunction, and aging hallmarks, are present in older humans and are associated with declining strength and cognition, as well as the development of sarcopenic obesity. Investigations on the origins of elevated OxS and mitochondrial dysfunction in older humans led to the discovery that deficiencies of the antioxidant tripeptide glutathione (GSH) and its precursor amino acids glycine and cysteine may be contributory. Supplementation with GlyNAC (combination of glycine and N-acetylcysteine as a cysteine precursor) was found to improve/correct cellular glycine, cysteine, and GSH deficiencies; lower OxS; and improve mitochondrial function, inflammation, insulin resistance, endothelial dysfunction, genotoxicity, and multiple aging hallmarks; and improve muscle strength, exercise capacity, cognition, and body composition. This review discusses evidence from published rodent studies and human clinical trials to provide a detailed summary of available knowledge regarding the effects of GlyNAC supplementation on age-associated defects and aging hallmarks, as well as discussing why GlyNAC supplementation could be effective in promoting healthy aging. It is particularly exciting that GlyNAC supplementation appears to reverse multiple aging hallmarks, and if confirmed in a randomized clinical trial, it could introduce a transformative paradigm shift in aging and geriatrics. GlyNAC supplementation could be a novel nutritional approach to improve age-associated defects and promote healthy aging, and existing data strongly support the need for additional studies to explore the role and impact of GlyNAC supplementation in aging.
Mainstream physicians are still hesitant to recommend low-carb diets because they are usually high in fat, potentially with heart-toxic levels of saturated fats. A recent scientific article supported low-carb eating for heart health.
Carbohydrate restriction shows promise for diabetes, but concerns regarding high saturated fat content of low-carbohydrate diets limit widespread adoption.Objectives
This preplanned ancillary study aimed to determine how diets varying widely in carbohydrate and saturated fat affect cardiovascular disease (CVD) risk factors during weight-loss maintenance.
Methods
After 10–14% weight loss on a run-in diet, 164 participants (70% female; BMI = 32.4 ± 4.8 kg/m2) were randomly assigned to 3 weight-loss maintenance diets for 20 wk. The prepared diets contained 20% protein and differed 3-fold in carbohydrate (Carb) and saturated fat as a proportion of energy (Low-Carb: 20% carbohydrate, 21% saturated fat; Moderate-Carb: 40%, 14%; High-Carb: 60%, 7%). Fasting plasma samples were collected prerandomization and at 20 wk. Lipoprotein insulin resistance (LPIR) score was calculated from triglyceride-rich, high-density, and low-density lipoprotein particle (TRL-P, HDL-P, LDL-P) sizes and subfraction concentrations (large/very large TRL-P, large HDL-P, small LDL-P). Other outcomes included lipoprotein(a), triglycerides, HDL cholesterol, LDL cholesterol, adiponectin, and inflammatory markers. Repeated measures ANOVA was used for intention-to-treat analysis.
Results
Retention was 90%. Mean change in LPIR (scale 0–100) differed by diet in a dose-dependent fashion: Low-Carb (–5.3; 95% CI: –9.2, –1.5), Moderate-Carb (–0.02; 95% CI: –4.1, 4.1), High-Carb (3.6; 95% CI: –0.6, 7.7), P = 0.009. Low-Carb also favorably affected lipoprotein(a) [–14.7% (95% CI: –19.5, –9.5), –2.1 (95% CI: –8.2, 4.3), and 0.2 (95% CI: –6.0, 6.8), respectively; P = 0.0005], triglycerides, HDL cholesterol, large/very large TRL-P, large HDL-P, and adiponectin. LDL cholesterol, LDL-P, and inflammatory markers did not differ by diet.
Conclusions
A low-carbohydrate diet, high in saturated fat, improved insulin-resistant dyslipoproteinemia and lipoprotein(a), without adverse effect on LDL cholesterol. Carbohydrate restriction might lower CVD risk independently of body weight, a possibility that warrants study in major multicentered trials powered on hard outcomes.
Parker here. These findings are no surprise to me.
Steve Parker, M.D.
PS: The Advanced Mediterranean Diet (2nd Ed.) includes a low-carb option.
Posted onJanuary 20, 2022|Comments Off on Mediterranean Ranked Diet #1 Again
Grapes are a time-honored component of the Mediterranean diet
From CNN:
It’s a winning streak that just won’t quit. For the fifth year in a row, the Mediterranean diet was first across the finish line in the annual race for best diet, according to ratings announced Tuesday by U.S. News & World Report.
Coming in a close second, in a tie: The DASH diet, which stands for dietary approaches to stop hypertension and emphasizes reducing salt intake; and the flexitarian diet, which encourages being a vegetarian most of the time — but is flexible enough to allow a burger once in a while
All three of these diets reduce or eliminate processed foods, and stress packing your plate with fruits, vegetables, beans, lentils, whole grains, nuts and seeds.
I’m surprised they ranked Atkins as the “Best Fast Weight-Loss Diet.” Looks like we’re getting over our collective phobia about saturated fat. “Keto Diet” ranked #4 in that category.
Now that you’ve blown your New Year’s weight-loss resolution, resolve to do better and try one of my diets! February 1 is a good start date.
Increasing numbers of physicians and the general public are starting to agree with Pardy.
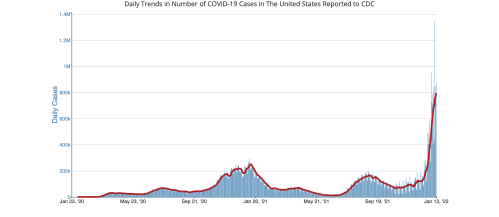
For most people, Omicron is a highly contagious cold. Lots will catch it, and most will get sniffles and a sore throat. Yes, even with Omicron, as with the flu, some people will get seriously ill, and a few will die. Masking, social distancing, capacity limits, lockdowns, curfews, and “vaccines” are not stopping the spread. People who dodge Omicron this time will face the next variant, or the one after that. Like other respiratory viruses in circulation, COVID-19 is here to stay.
Therefore, COVID is done. Either mild Omicron is the end of COVID madness, or there is no off-ramp.
Will the next SARS-CoV-2 variant be more or less virulent than omicron? Only time will tell. From the start of this pandemic, some virologists were saying that the natural history of these viruses is to become less virulent as they evolve.
Have you noticed we don’t have vaccines for the common cold? Either the scientists don’t know how to make an effective one, or it’s just not worth the cost of development and deployment. Not to mention the medical risks of vaccines. For all we know, it’s good for us to fight off a common cold once or twice a year. Keeps our immune system tuned up.
Seeing the public’s hair-on-fire response to the national lack of testing over the last week, I’m wondering if we all really need to be tested for COVID-19 when we have symptoms. We don’t all run to the doctor when we have a head cold or viral bronchitis or laryngitis. Those are transmittable to those around you. If you’re sick with those, don’t go to work. Avoid others and take precautions to protect them if un-avoidable. Especially stay away from the elderly and those with poor immune systems or illnesses that would increase the risk of death if they caught your infection. The folks who truly need a reliable COVID-19 test when symptomatic are the candidates for early outpatient anti-viral treatment, such as the elderly and others at high risk for serious COVID-19.
IIRC, the CDC says there’s no need for a repeat COVID-19 PCR test to prove you’re no longer infectious to others. As long as you’re five (or ten?) days out from your last fever or symptoms, you are unlikely to be shedding infectious virus. But you can shed non-infectious viral debris that PCR can detect for up to 12 weeks after illness resolution.
Now the World Health Organization has waved the white flag on Covid vaccine boosters too.
WHO released a statement about Covid vaccines yesterday. It’s filled with the usual public health jargon and ass-covering, but one line stands out:
a vaccination strategy based on repeated booster doses of the original vaccine composition is unlikely to be appropriate or sustainable.
It’s over, people.
Aside from a few unlucky Israelis, no one is going to receive a fourth dose of the original vaccine; everyone with eyes can see it doesn’t work against Omicron. (And if you haven’t gotten a third dose, at this point, why would you? You are getting at most weeks of marginally improved protection for potentially severe side effects.)
When asked who they trusted to provide information about COVID-19 only 30.8 percent said Fauci, Biden’s chief medical adviser, and 15.5 percent said Biden himself.
Instead, almost two thirds said they trusted their doctor for advice, and almost half said they trusted federal health authorities such as the Centers for Disease Control and Prevention.
Only the news media fared worse than Biden and his top adviser, with barely 10 percent saying they trusted journalists.
The Stalinist-era Soviet Union was notorious for stripping dissidents of their professional credentials and subjecting them to psychiatric inquisitions. Today, the USA is following in the USSR’s footsteps. An early victim—and a canary in the proverbial coal mine—is Maine physician Meryl Nass.
On January 11 Maine’s Board of Licensure in Medicine suspended Dr. Nass’s license and ordered her to undergo a psychiatric exam, stating: “In the interests of public health and safety the Board may compel a physician to submit to a mental or physical examination upon a complaint or allegation that the physician is or may be unable to practice medicine with reasonable skill and safety to patients by reason of a mental illness, alcohol intemperance, excessive use of drugs narcotics, or as a result of a mental or physical condition interfering with the competent practice of medicine.”
Dr. Nass is not a drug or alcohol abuser. She is obviously perfectly sane. Indeed, she is uncommonly lucid and articulate….
As a complement to vaccines, small-molecule therapeutic agents are needed to treat or prevent infections by severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) and its variants, which cause COVID-19. Affinity selection-mass spectrometry was used for the discovery of botanical ligands to the SARS-CoV-2 spike protein. Cannabinoid acids from hemp (Cannabis sativa) were found to be allosteric as well as orthosteric ligands with micromolar affinity for the spike protein. In follow-up virus neutralization assays, cannabigerolic acid and cannabidiolic acid prevented infection of human epithelial cells by a pseudovirus expressing the SARS-CoV-2 spike protein and prevented entry of live SARS-CoV-2 into cells. Importantly, cannabigerolic acid and cannabidiolic acid were equally effective against the SARS-CoV-2 alpha variant B.1.1.7 and the beta variant B.1.351. Orally bioavailable and with a long history of safe human use, these cannabinoids, isolated or in hemp extracts, have the potential to prevent as well as treat infection by SARS-CoV-2.
Posted onJanuary 15, 2022|Comments Off on Merck’s COVID-19 Pill: Molnupiravir
“I’m so sorry. We don’t have that in stock. But we have ivermectin!”
On Dec 23, 2021, FDA gave Emergency Use Authorization to molnupiravir as outpatient treatment for COVID-19 in high-risk patients 18 and older. “High risk” means high risk for hospitalization or death from COVID-19. Users need a positive COVID-19 test and should start treatment as early as possible, within five days of symptom onset.
The drug reduced hospitalization and death by 30%. FDA approval was based on a clinical study that included only ~700 patients who got the pill. I assume there were 700 others who got a placebo.
By comparison, Pfizer’s Paxlovid reduced hospitalization and death by 90%.
The dose is 800 mg by mouth every 12 hours for five days. Available capsules contain 200 mg.
Notes:
The drug is well-tolerated. Most common side effects are diarrhea, nausea, and dizziness.
No known drug interactions. This is an advantage over Pfizer’s Paxlovid pill.
No dose adjustment needed for kidney disease, liver disease, or old age. Another advantage over Paxlovid.
The drug could be dangerous to embryos/fetuses. Don’t get pregnant while taking this! Male users need to use reliable birth control for the three months after use.
“If you’re looking to improve your heart health, you may want to try eating a low-carb, high-fat Mediterranean diet. Why? Because a new study published in The American Journal of Clinical Nutrition found that eating a low-carb (no more than 20% of daily calories from carbs), the high fat-style Mediterranean diet may reduce the risk of cardiovascular disease (CVD). For the study, obese study participants reported both improved insulin resistance and cholesterol levels compared to those who ate a moderate carb (40%) or high carb (60%) diet over a five-month period.”
Steve Parker, M.D.
PS: The Ketogenic Mediterranean Diet is obviously low-carb, and is included in both The Advanced Mediterranean Diet (2nd Ed.) and Conquer Diabetes and Prediabetes.
Posted onJanuary 12, 2022|Comments Off on Acetaminophen: Should It Be Used in COVID-19 and Other Infections?
This article may trigger your insomnia
Acetaminophen is a very common drug used to relieve pain and reduce fever. A few of its advantages over non-steroidal anti-inflammatory drugs are that it rarely causes bleeding, upset stomach, or kidney impairment. In excessive doses, acetaminophen causes liver toxicity. The most common brand name is Tylenol.
Last year I watched a video of ZDoggMD and Dr Marty Makarey wherein the latter mentioned offhand that acetaminophen (aka paracetamol) worsens the effect of cytokine storm in COVID-19. That was news to me.
First, note that antioxidant activity is considered an important defense against inflammation, including that which might be due to infection. An important player in antioxidant activity is glutathione. Acetaminophen apparently and commonly reduces blood and cellular glutathione levels. Hence, less antioxidant activity leading to worse infection outcomes. That’s the theory anyway. This is one article that supports Makarey’s remark.
You may have heard about NAC (N-acetylcysteine) being used as a treatment for COVID-19. NAC is a precursor to glutathione.
Guess what the antidote for acetaminophen poisoning is…NAC
From the article linked above:
GSH [glutathione], an abundant tripeptidyl molecule, contributes to the body and lung health status (Cantin and Begin, 1991) and plays pivotal roles in protecting cells against oxidative stress-induced cellular damage, in detoxifying xenobiotics and drug metabolism (Cantoni et al., 1996); decreased GSH levels are associated with the common features of aging as well as of a wide range of pathological conditions (Homma and Fujii, 2015), comorbidities, smoking habit which, intriguingly, represent the major risk factors for COVID-19.
Resistance to viral diseases positively correlates with the extent of GSH stores (Khomich et al., 2018). Higher levels of GSH have been associated with better individual’s responsiveness to viral infections (De Flora et al., 1997; Lee, 2018): in particular, GSH is known to protect host immune cells operating in oxidative stressing environments and contributes to their optimal functioning. Reactive oxygen species (ROS)-induced alterations of the immune response has been proposed as a key player in COVID-19 pathogenesis and antioxidant intervention with NAC recommended as a preventive and therapeutic strategy (De Flora et al., 2020; Schönrich et al., 2020).
Interestingly, preventive supplementation of NAC significantly reduced the incidence of clinically apparent influenza, especially in higher risk elderly population (De Flora et al., 1997). This effect may also depend on the GSH-induced inhibition of various respiratory viruses’ replication, an effect which is thought to prevent increased viral loads and the subsequent massive release of inflammatory cells into the lung. i.e. cytokine storm (Palamara et al., 1996; Nencioni et al., 2003). To this regard, GSH may also have direct anti-SARS-CoV-2 potential: indeed a computational study indicates that the binding of spike protein to ACE2 is maximal when ACE2-sulfur groups are in the form of disulfides and impaired when fully reduced to thiols: hence a prooxidant environment with low levels of GSH would favor viruses cellular entry (Hati and Bhattacharyya, 2020).
One of the authors’ conclusions is:
The routinary use of PAC [paracetamol, aka acetaminophen] in at risk categories, along with their intrinsically frail conditions, may have further worsen the scarcity of GSH, especially in western countries where PAC consumption is particularly high. Such a situation may have rendered this group of population even more susceptible to SARS-CoV2 at the time of its spreading. To this end a merely speculative but intriguing hypothesis is that PAC adoption might have contributed to the high virulence of COVID-19 observed in many EU countries and USA. Notably, in most countries PAC is freely sold as an OTC [over the counter] drug, raising the risk of unintentional abuse and increased adverse effects (Sansgiry et al., 2017).
Interesting stuff. But at this point there is no medical consensus on this issue.
“Daily consumption for nuts and seeds was associated with a lower prevalence of NAFLD in non-Mediterranean, US adults, although the benefits seem to be greater in females across all categories of nut and seed consumption groups compared with nonconsumers. Both males and females presented with lower prevalence of NAFLD with intakes of 15–30 g/d.”