Posted onMarch 11, 2022|Comments Off on Green-Mediterranean Diet Out-Performed the Mediterranean Diet for Loss of Liver Fat
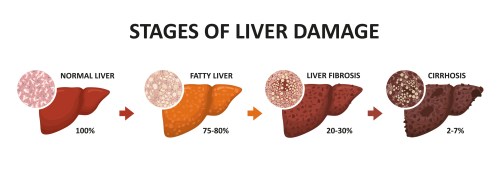
Stages of liver damage. Healthy, fatty, liver fibrosis and cirrhosis
About one quarter of the world’s adults have excess fat accumulation in the the liver called non-alcoholic fatty liver disease (NAFLD). This can lead to liver inflammation, scarring (cirrhosis), and liver cancer. The adverse effects of liver fat can be prevented by loss of that fat. The most common medical recommendation to accomplish that is to loss excess body weight via any reasonable method.
A study published in Gut last year found greater reduction in liver fat in those eating a “green-Mediterranean” diet compared to a regular Mediterranean diet over 18 months. Both diets were supplemented with walnuts 28 grams/day. Details of the green-Med diet:
In addition to [physical activity] and the provision of 28 g/day walnuts, the green-MED diet was restricted in processed and red meat and was richer in plants and polyphenols. The participants were guided to further consume the following provided items: 3–4 cups/day of green tea and 100 g/day of frozen Wolffia globosa (Mankai strain) plant frozen cubes, as a green shake replacing dinner. Both green tea and Mankai together provided additional daily intake of 800 mg polyphenols ((GAE), according to Phenol-Explorer and Eurofins lab analysis, including catechins (flavanols)) beyond the polyphenol content in the prescribed MED diet. Both the MED and green-MED diets were equally calorie-restricted (1500–1800 kcal/day for men and 1200–1400 kcal/day for women).
The researchers don’t tell us where to get frozen Wolffia globosa (Mankai strain) plant frozen cubes.
Study participants were almost all men, so results may not apply to women.
We are meeting at a difficult time, when our Armed Forces are conducting a special military operation in Ukraine and Donbas. Let me remind you that at the very beginning of it, in the early morning of February 24, I publicly and openly named the reasons and the main goal of Russia’s actions. This is assistance to our people in the Donbas, who for almost eight years were subjected to real genocide by the most barbaric methods – blockade, large-scale punitive actions, terrorist attacks and constant artillery shelling. And for what? Only for the fact that they sought basic human rights – to live according to the laws and traditions of their ancestors, to speak their native language, to raise their children the way they want.
At the same time, the Kiev authorities not only ignored and sabotaged the implementation of the Minsk Package of Measures for the Peaceful Settlement of the Crisis throughout all these years, but at the end of last year they publicly refused to implement it altogether.
They have also begun to put into practice plans to join NATO. Moreover, there were also statements by the Kiev authorities about their intention to create their own nuclear weapons and their means of delivery. It was a real threat. Already in the foreseeable future, with foreign technical assistance, the pro-Nazi regime in Kiev could get its hands on weapons of mass destruction, and the target for it, of course, would be Russia.
In Ukraine, there was also a network of dozens of laboratories where military biological programs were conducted under the leadership and with the financial support of the Pentagon, including experiments with samples of coronavirus, anthrax, cholera, African swine fever and other deadly diseases. Traces of these secret programs are now being intensively tried to cover up. But we have every reason to believe that in the immediate vicinity of Russia, on the territory of Ukraine, in fact, biological weapons components were created.
Our repeated warnings that such a development poses a direct threat to Russia’s security have been rejected by Ukraine and its patrons in the United States and NATO, with ostentatious and cynical disdain.
Thus, all diplomatic options were completely exhausted. We were simply left with no options to peacefully solve problems that arise through no fault of our own. And in this regard, we were simply forced to launch a special military operation.
The appearance of Russian troops near Kiev and other cities of Ukraine is not connected with the intention to occupy this country. We do not have such a goal, and I also explicitly stated this in my address on February 24.
As for the tactics of combat operations, which were developed by the Ministry of Defense of Russia and our General Staff, they have fully justified themselves. And our guys – soldiers and officers – show courage and heroism, do everything that depends on them to avoid losses among the civilian population of Ukrainian cities.
I want to say this for the first time: at the very beginning of the operation in the Donbas, the Kiev authorities were asked through various channels, in order to avoid senseless bloodshed, not to enter into hostilities, but simply to withdraw their troops from the Donbass. They didn’t want to. Well, that’s their decision. Awareness of what is happening in the real world, on the ground, will inevitably come.
The operation is developing successfully, in strict accordance with pre-approved plans.
I would like to note that Ukraine, encouraged by the United States and a number of Western countries, purposefully prepared for a scenario of force, carnage and ethnic cleansing in Donbass. A massive offensive into the Donbas and then crimea was only a matter of time. And our Armed Forces foiled these plans.
Kiev was not only preparing for war, for aggression against Russia, against Donbass– they were fighting it. Attempts to organize sabotage and terrorist underground in Crimea did not stop. In recent years, hostilities have continued in the Donbas, shelling of peaceful settlements. During this time, almost 14,000 civilians were killed, among them children.
I want ordinary citizens of Western countries to hear me: they [Western leaders and media?] are now persistently trying to convince you that all your difficulties are the result of some hostile actions of Russia, that from your own wallet you need to pay for the fight against the mythical Russian threat. It’s all a lie.
The truth is that the current problems faced by millions of people in the West are the result of years of actions by the ruling elites of their states, their mistakes, short-sightedness and ambition. These elites are not thinking about how to improve the lives of their citizens in countries. They are obsessed with their vested interests and super-profits.
Evidence of this is the data of international organizations that directly say that social problems, even in the leading Western countries, have only worsened in recent years, that inequality, the gap between the rich and poor are growing, racial and national conflicts are making themselves felt. The myth of a Western welfare society, of the so-called golden billion, is crumbling.
Let me repeat that today the entire planet has to pay precisely for the ambitions of the West, for its attempts by any means to maintain its elusive dominance.
Evidence of this is the data of international organizations that directly say that social problems, even in the leading Western countries, have only worsened in recent years, that inequality, the gap between the rich and poor are growing, racial and national conflicts are making themselves felt. The myth of a Western welfare society, of the so-called golden billion, is crumbling.
Let me repeat that today the entire planet has to pay precisely for the ambitions of the West, for its attempts by any means to maintain its elusive dominance.
The imposition of sanctions is a logical continuation, a concentrated expression of the irresponsible, short-sighted policies of the governments and central banks of the United States and the EU countries. In recent years, it has been they who have dispersed the spiral of global inflation with their own hands, led to the growth of global poverty and increased inequality, to new flows of refugees around the world. And this begs the question: Who will now be responsible for the millions of starvation deaths in the world’s poorest countries due to growing food shortages?
I repeat, a serious blow has been dealt to the entire global economy and trade, to confidence in the US dollar as the main reserve currency.
Thus, illegitimate actions to freeze part of the Bank of Russia’s foreign exchange reserves draw a line under the reliability of so-called first-class assets. In fact, both the United States and the EU have declared a real default on their obligations to Russia. Now everyone knows that financial reserves can simply be stolen. And seeing this, many countries in the near future can begin – I am sure that this will happen – to convert their paper and digital savings into real reserves in the form of commodities, land, food, gold, and other real assets, which will only increase the deficit in these markets.
Propaganda? Yes, maybe. You’re seeing propaganda from all sides if you’re paying attention.
Without a declaration of war from Congress, President Biden is using my and your tax dollars to send war-fighting materiel to Ukraine. Hey, Brandon, how about addressing U.S. citizens as to what exactly is our vital national interest in Ukraine?
The great rule of conduct for us in regard to foreign nations is, in extending our commercial relations, to have with them as little political connection as possible.
“It is our true policy to steer clear of permanent alliance with any portion of the foreign world”: it was George Washington’s Farewell Address to us. The inaugural pledge of Thomas Jefferson was no less clear: “Peace, commerce, and honest friendship with all nations – entangling alliances with none.”
Viagra (one brand name for generic sildenafil) is used to treat erectile dysfunction and pulmonary hypertension. I bet that usage for ED is far more common than for pulmonary hypertension.
…the team analyzed insurance claims data from more than 7 million Americans. They found that the people (mostly men) who took sildenafil were 69% less likely to develop AD [Alzheimer’s Disease] over 6 years than those who did not take the drug. This association between sildenafil and AD held after adjusting for sex, age, and other diseases and conditions.
To understand how sildenafil might affect AD, the researchers grew neurons from stem cells derived from AD patients. Exposing the cells to sildenafil led to increased growth of neurites, which connect neurons to each other, and decreased tau phosphorylation, an early biomarker of AD.
Taken together, these results show an association between sildenafil use and reduced AD risk. But the researchers emphasize that they haven’t shown that sildenafil prevents or reverses AD.
These things usually don’t pan out, but one can hope. How often were these guys taking viagra? Once a month? Twice a week? To treat erectile dysfunction, sildenafil is typically taken as needed one hour before sexual activity. Typical dose for pulmonary hypertension is 20 mg by mouth three times a day, every day. Would this drug affect dementia in women? As they say, further studies are needed.
Posted onFebruary 26, 2022|Comments Off on Ultra-Processed Foods ——> Higher Coronary Artery Disease Risk
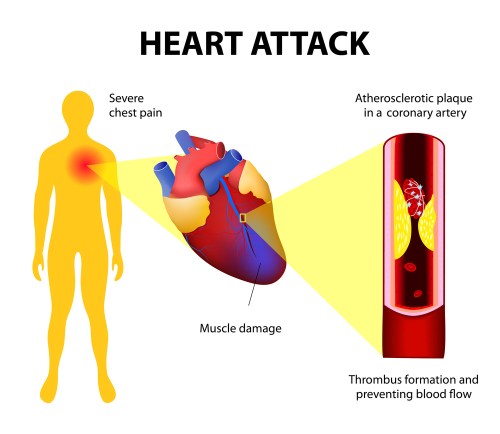
Heart attacks and chest pains are linked to blocked arteries in the heart (coronary artery disease)
What are ultra-processed foods? I’m not paying $35 for the scientific article to find out. If you can grab the definition from your copy, please share in the Comments section. The 2020 profit from my publishing company was only $937.08, so I’m watching my expenses.
Here’s the free abstract:
ABSTRACT
Background
Higher ultra-processed food intake has been linked with several cardiometabolic and cardiovascular diseases. However, prospective evidence from US populations remains scarce.
Objectives
To test the hypothesis that higher intake of ultra-processed foods is associated with higher risk of coronary artery disease.
Ultra-processed versus processed?
Methods
A total of 13,548 adults aged 45–65 y from the Atherosclerosis Risk in Communities study were included in the analytic sample. Dietary intake data were collected through a 66-item FFQ. Ultra-processed foods were defined using the NOVA classification, and the level of intake (servings/d) was calculated for each participant and divided into quartiles. We used Cox proportional hazards models and restricted cubic splines to assess the association between quartiles of ultra-processed food intake and incident coronary artery disease.
Results
There were 2006 incident coronary artery disease cases documented over a median follow-up of 27 y. Incidence rates were higher in the highest quartile of ultra-processed food intake (70.8 per 10,000 person-y; 95% CI: 65.1, 77.1) compared with the lowest quartile (59.3 per 10,000 person-y; 95% CI: 54.1, 65.0). Participants in the highest compared with lowest quartile of ultra-processed food intake had a 19% higher risk of coronary artery disease (HR: 1.19; 95% CI: 1.05, 1.35) after adjusting for sociodemographic factors and health behaviors. An approximately linear relation was observed between ultra-processed food intake and risk of coronary artery disease.Conclusions
Higher ultra-processed food intake was associated with a higher risk of coronary artery disease among middle-aged US adults. Further prospective studies are needed to confirm these findings and to investigate the mechanisms by which ultra-processed foods may affect health.
I admit I must eat some ultra-processed foods, but try to limit them.
Heart disease is the #1 killer in the developed world, even more lethal the COVID19! If you’ve abandoned your New Years’ weight-loss diet, consider one low in ultra-processed foods, like the Mediterranean diet.
Greek salad with canned salmon. Salmon is rich in heart-healthy omega-3 fatty acids.
Posted onFebruary 24, 2022|Comments Off on COVID-19 Link Dump: Did the Queen Take Ivermectin? COVID as STI, Long COVID Risk Factors, Ivermectin Failure?
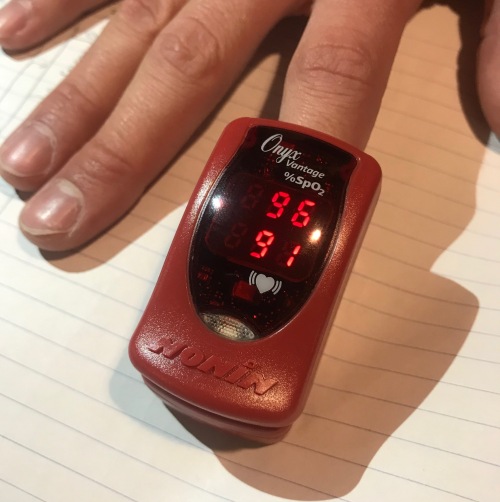
Is O2 saturation of 80-85% good enough without intubating some folks? 91 = heart rate.
Oral ivermectin 400 mcg/kg daily for five days did not prevent progression to severe disease, defined as a requirement of supplemental oxygen at achieve oxygen saturation of at least 95%. The study included ~250 folks on ivermectin versus the “standard care” comparison group. The definition of an adequate oxygen saturation level is a matter of debate among physician experts. Where I work, you’re generally not going to be admitted to the hospital or given supplemental oxygen if your O2 sat is under 92. Other physicians or institutions worry if your O2 sat is 94% or less, and define “severe” COVID-19 as having an O2 sat 94% or less.
The study authors conclude: In this randomized clinical trial of high-risk patients with mild to moderate COVID-19, ivermectin treatment during early illness did not prevent progression to severe disease. The study findings do not support the use of ivermectin for patients with COVID-19.
Posted onFebruary 23, 2022|Comments Off on Yet Another Study Supports the Life-Preserving Effect of the Mediterranean Diet
Cardiovascular diseases include heart attacks and strokes. Those are major killers. So it’s good to know about dietary habits that counteract the threat.
Examining a variety of diet quality methodologies will inform best practice use of diet quality indices for assessing all-cause and CVD [cardiovascular disease] mortality.
Objective
To examine the association between three diet quality indices (Australian Dietary Guideline Index, DGI; Dietary Inflammatory Index, DII; Mediterranean-DASH Intervention for Neurodegenerative Delay, MIND) and risk of all-cause mortality, CVD mortality and non-fatal CVD events up to 19 years later.Design
Data on 10,009 adults (51.8 years; 52% female) from the Australian Diabetes, Obesity and Lifestyle study were used. A food frequency questionnaire was used to calculate DGI, DII and MIND at baseline. Cox proportional hazard models were used to estimate hazard ratios (HR) and 95% CI of all-cause mortality, CVD mortality and non-fatal CVD events (stroke; myocardial infarction) according to 1 SD increase in diet quality, adjusted for age, sex, education, smoking, physical activity, energy intake, history of stroke or heart attack, and diabetes and hypertension status.Results
Deaths due to all-cause (n = 1,955) and CVD (n = 520), and non-fatal CVD events (n = 264) were identified during mean follow-ups of 17.7, 17.4 and 9.6 years, respectively. For all-cause mortality, HRs associated with higher DGI, DII and MIND were 0.94 (95% CI: 0.89, 0.99), 1.08 (95% CI: 1.02, 1.15) and 0.93 (95% CI: 0.89, 0.98), respectively. For CVD mortality, HRs associated with higher DGI, DII and MIND were 0.93 (95% CI: 0.85, 0.99), 1.10 (95% CI: 1.00, 1.24) and 0.90 (95% CI: 0.82, 0.98), respectively. There was limited evidence of associations between diet quality and non-fatal CVD events.Conclusions
Better quality diet predicted lower risk of all-cause and CVD mortality in Australian adults, while a more inflammatory diet predicted higher mortality risk. These findings highlight the applicability of following Australian dietary guidelines, a Mediterranean style diet and a low-inflammatory diet for the reduction of all-cause and CVD mortality risk.
Posted onFebruary 14, 2022|Comments Off on Low-Calorie Mediterranean Diet May Healthier Than High-Protein Non-Mediterranean?
One of many ketogenic salads
Researchers compared three low-calorie diets and concluded that the Mediterranean option was the healthiest. The study at hand today is way too small to be considered anything but a pilot study. So results may not be replicable on a larger scale. I’d like to know how compliant study subjects were with the protocol, because 700 calories a day for six weeks is quite a challenge.
Comparison of short-term hypocaloric high-protein diets with a hypocaloric Mediterranean diet: Effect on body composition and health-related blood markers in overweight and sedentary young participants
Highlights
A hypocaloric Mediterranean diet provides all the necessary nutrients.
The hypocaloric Mediterranean diet reduces body mass and fat mass and maintains fat-free mass.
The hypocaloric Mediterranean diet is beneficial on metabolic and inflammation/muscle- damage indices.
Hypocaloric high-protein diets with and without whey supplementation reduce body mass and fat-free mass but not fat mass.
Hypocaloric high-protein diets with and without whey supplementation are adverse on metabolic and inflammation/muscle-damage indices
Abstract
Objectives
The aim of the present study was to compare the short-term effects of a hypocaloric Mediterranean diet and two high protein diets, with and without whey protein supplementation, on body composition, lipidemic profile, and inflammation and muscle-damage blood indices in overweight, sedentary, young participants.
Methods
Thirty-three young, overweight, male and female participants (mean ± SD age: 22.8 ± 4.8 y; body mass: 85.5 ± 10.2 kg; body fat percentage: 34.3% ± 8.1%) were randomly allocated to three different hypocaloric (−700 kcal/d) diets: a Mediterranean diet (MD; n = 10), a high-protein diet (HP; n = 10) diet, and a high-protein diet with whey supplementation (n = 10). The intervention lasted 6 wk. Body composition and biochemical indices were evaluated 1 wk before and after the nutritional interventions.
Results
Body and fat mass were decreased in the MD and HP groups (−3.5% ± 1.1% and −5.9% ± 4.2% for body and fat mass respectively in MD, and −1.7% ± 1.2% and −2.0% ± 1.8% for body and fat mass respectively in HP;P < 0.05), with no significant decline of fat-free mass observed in the MD group. The MD group’s diet beneficially altered the lipid profile (P < 0.05), but the HP and HPW groups’ diets did not induce significant changes. Subclinical inflammation and muscle-damage indices significantly increased in the HP and HPW groups (7.4% ± 3.5% and 66.6% ± 40.1% for neutrophils and CRP respectively in HP, and 14.3% ± 6.4% and 266.6% ± 55.1% for neutrophils and CRP respectively in HPW; P < 0.05) but decreased in the MD group (1.8% ± 1.2% and −33.3% ± 10.1% for neutrophils and CRP respectivelyc; P < 0.05). Energy intake of carbohydrates and proteins were significantly related to the changes in body composition and biochemical blood markers (r = −0.389 and −0.889; P < 0.05).
Conclusions
Among the three hypocaloric diets, only the Mediterranean diet induced positive changes in body composition and metabolic profile in overweight, sedentary individuals.
I’ve got to get something off my chest, so buckle up for an overdue rant.
I can’t begin to describe the disdain and contempt I have for highly-credentialed MD’s with large platforms who are suddenly jumping on the Team Reality about COVID-19.
…
If we are getting out of this mess it won’t be due to MDs. They’ve abdicated their roles because most no longer are in practice for themselves and must rely on CMS [Medicare] dollars. Whoever pays the salary makes the rules.
It’s not only “highly-credentialed MD’s” who deserve disdain and contempt.
It’s not just a list. Steve tells you why they made the cut. See also his list of top corporate misinformation spreaders, if you dare. The article is a concise summary of who’s to blame for the mismanagement of this pandemic. (Or was it managed precisely how our overlords wanted it?)
“Your neighbor reported you for dissing Fauci! On your knees NOW, kulak!” Photo by Somchai Kongkamsri on Pexels.com
The United States remains in a heightened threat environment fueled by several factors, including an online environment filled with false or misleading narratives and conspiracy theories, and other forms of mis- dis- and mal-information (MDM) introduced and/or amplified by foreign and domestic threat actors. These threat actors seek to exacerbate societal friction to sow discord and undermine public trust in government institutions to encourage unrest, which could potentially inspire acts of violence. Mass casualty attacks and other acts of targeted violence conducted by lone offenders and small groups acting in furtherance of ideological beliefs and/or personal grievances pose an ongoing threat to the nation. While the conditions underlying the heightened threat landscape have not significantly changed over the last year, the convergence of the following factors has increased the volatility, unpredictability, and complexity of the threat environment: (1)the proliferation of false or misleading narratives, which sow discord or undermine public trust in U.S. government institutions; (2) continued calls for violence directed at U.S. critical infrastructure; soft targets and mass gatherings; faith-based institutions, such as churches, synagogues, and mosques; institutions of higher education; racial and religious minorities; government facilities and personnel, including law enforcement and the military; the media; and perceived ideological opponents; and (3) calls by foreign terrorist organizations for attacks on the United States based on recent events.
#1 among factors contributing to heightened threat risk:
The proliferation of false or misleading narratives, which sow discord or undermine public trust in U.S. government institutions:
For example, there is widespread online proliferation of false or misleading narratives regarding unsubstantiated widespread election fraud and COVID-19. Grievances associated with these themes inspired violent extremist attacks during 2021. [Huh?]
Thank God the threat expires at 1400 hrs June 7, 2022. How will I ever sleep at night until then.
Never forget, comrades, that our governments and gov’t institutions can do no wrong. So don’t criticize them or you may be visited by the FBI. Or worse.
Are you willing to consider that most everything you learned about Abe Lincoln in school is wrong? Or would that be too mind-blowing? Reading Ilana Mercer’s article be the start of your red-pilling adventure:
Today is Abraham Lincoln’s birthday. Familiar Lincoln idolaters will gather to celebrate the birth, on Feb. 12, 1809, of the 16th President of the United States, and finesse his role in “the butchering business”—to use Prof. J. R. Pole’s turn-of-phrase. Court historian Doris Kearns Goodwin is sure to make a media appearance to extol the virtues of the president who shed the blood of brothers in great quantities, and urged into existence the “American System” of taxpayer-sponsored grants of government privilege to politically connected corporations.
On publication, in 2002, of the book “The Real Lincoln: A New Look at Abraham Lincoln, His Agenda, and an Unnecessary War,” the “Church of Lincoln” gave battle. The enemy was the author, Thomas J. DiLorenzo, who had exposed Lincoln lore for the lie it was — still is. DiLorenzo had dared to examine the “Great Centralizer’s” role in sundering the soul of the American federal system: the sovereignty of the states and the citizenry.
Remember, the victors of war write the history books.
Steve Parker, M.D.
PS: I’ve not studied this aspect of American history in detail. DiLorenzo’s book has been on my “to be read” list for 15 years. One of these days….
Posted onJanuary 30, 2022|Comments Off on COVID-19 Link Dump: Rapid Diagnostic Tests, Ivermectin Works, Vax Adverse Effects, Life Insurance Doesn’t Pay for Suicide, Senator Johnson’s COVID-19 Panel, Kirsch Interviews Healthcare Workers
Do some nurses really call remdesivir, “run, death is near”?
Many drugstores and others in the U.S. are now selling over-the-counter home testing kits for “diagnosis” of COVID-19. My wife brought home a sack full of them (Flowflex made in China) for ~$8 a pop. Three months ago, CVS was selling a home test kit for $40. The Flexflow box said it was “accurate,” but not how accurate. How should these and other “rapid” diagnostic tests be used? Dr Paul Drain offers advice in NEJM: Rapid Diagnostic Testing for SARS-CoV-2
This is not easy reading unless you’re smart or have medical background.
Prophylactic ivermectin significantly reduced infections, hospitalizations, and deaths from COVID-19 in Brazil. But that would never work here, right?
Background: Ivermectin has demonstrated different mechanisms of action that potentially protect from both coronavirus disease 2019 (COVID-19) infection and COVID-19-related comorbidities. Based on the studies suggesting efficacy in prophylaxis combined with the known safety profile of ivermectin, a citywide prevention program using ivermectin for COVID-19 was implemented in Itajaí, a southern city in Brazil in the state of Santa Catarina. The objective of this study was to evaluate the impact of regular ivermectin use on subsequent COVID-19 infection and mortality rates.
In the absence of contraindications, ivermectin was offered as an optional treatment to be taken for two consecutive days every 15 days at a dose of 0.2 mg/kg/day.
Results: Of the 223,128 citizens of Itajaí considered for the study, a total of 159,561 subjects were included in the analysis: 113,845 (71.3%) regular ivermectin users and 45,716 (23.3%) non-users. Of these, 4,311 ivermectin users were infected, among which 4,197 were from the city of Itajaí (3.7% infection rate), and 3,034 non-users (from Itajaí) were infected (6.6% infection rate), with a 44% reduction in COVID-19 infection rate (risk ratio [RR], 0.56; 95% confidence interval (95% CI), 0.53-0.58; p < 0.0001). Using PSM, two cohorts of 3,034 subjects suffering from COVID-19 infection were compared. The regular use of ivermectin led to a 68% reduction in COVID-19 mortality (25 [0.8%] versus 79 [2.6%] among ivermectin non-users; RR, 0.32; 95% CI, 0.20-0.49; p < 0.0001). When adjusted for residual variables, reduction in mortality rate was 70% (RR, 0.30; 95% CI, 0.19-0.46; p < 0.0001). There was a 56% reduction in hospitalization rate (44 versus 99 hospitalizations among ivermectin users and non-users, respectively; RR, 0.44; 95% CI, 0.31-0.63; p < 0.0001). After adjustment for residual variables, reduction in hospitalization rate was 67% (RR, 0.33; 95% CI, 023-0.66; p < 0.0001).
Conclusion: In this large PSM study, regular use of ivermectin as a prophylactic agent was associated with significantly reduced COVID-19 infection, hospitalization, and mortality rates.
Once Dr David Gorski sees Pierre Kory’s name among the authors, I’m sure he’ll rip this study to shreds.
Don’t forget that the FDA never could have issued Emergency Use Authorizations for vaccines and many current drugs if they admitted there was already a single existing effect therapy or prevention for COVID-19.
Although vaccination is recognized as the cause of death by doctors and the insurance company, it has refused to pay out. The reason is because the side effects of the Corona jabs are known and published. They argue that the deceased took part in an experiment at his own risk.
The insurance company justified the refusal of payment to the family by stating that the use of experimental medication or treatments, including Corona injections, is expressly excluded from the insurance contract. The family’s subsequent lawsuit against the insurance company has been unsuccessful.
The court allegedly justified its ruling as follows: “The side effects of the experimental vaccine are published and the deceased could not claim to have known nothing about it when he voluntarily took the vaccine. There is no law or mandate in France that compelled him to be vaccinated. Hence his death is essentially suicide.” Since suicide is not covered by the policy from the outset, the insurance refuses to budge.
On January 24, 2022 Senator Ron Johnson invited a group of world renowned doctors and medical experts to the U.S. Senate to provide a different perspective on the global pandemic response, the current state of knowledge of early and hospital treatment, vaccine efficacy and safety, what went right, what went wrong, what should be done now, and what needs to be addressed long term. This 38 minute video highlights the 5-hour discussion.
Comments Off on COVID-19 Link Dump: Rapid Diagnostic Tests, Ivermectin Works, Vax Adverse Effects, Life Insurance Doesn’t Pay for Suicide, Senator Johnson’s COVID-19 Panel, Kirsch Interviews Healthcare Workers